A SYSTEMATIC APPROACH TO WEIGHT LOSS, DISEASE MANAGEMENT & PREVENTION, IN A HEALTH CARE PRACTICE.
LIFESTYLENUTRITIONINC.COM – For Doctors or 800-699-8106
The Problem
As practicing MD for 17 years, traditionally, providing patients with individualized nutritional counseling guidelines for weight loss, diabetes, pre-diabetes, hyperlipidemias and other clinical meal plans have been challenging and ineffective. Eighty percent of our patients want to eat healthier, exercise more, lose weight & learn how to decrease their disease risks with food & lifestyle rather than just with medications. As busy practitioners, we don’t have time to put together a personal nutrition and exercise programs So ,on a daily basis, we provide generic pharmaceutical diet handouts to many of our patients. generic diet sheets are either too general or too restrictive and are not customized for patients food preferences and lifestyle. As a result, patient compliance is poor and then we feel our patients are not receptive to making any diet or lifestyle changes. We have also tried using, meal replacements, packaged foods, meds and or hormones which provided short-term results, at best and also did not focus on a patient’s lifestyle, metabolism, and individual food preferences
Background
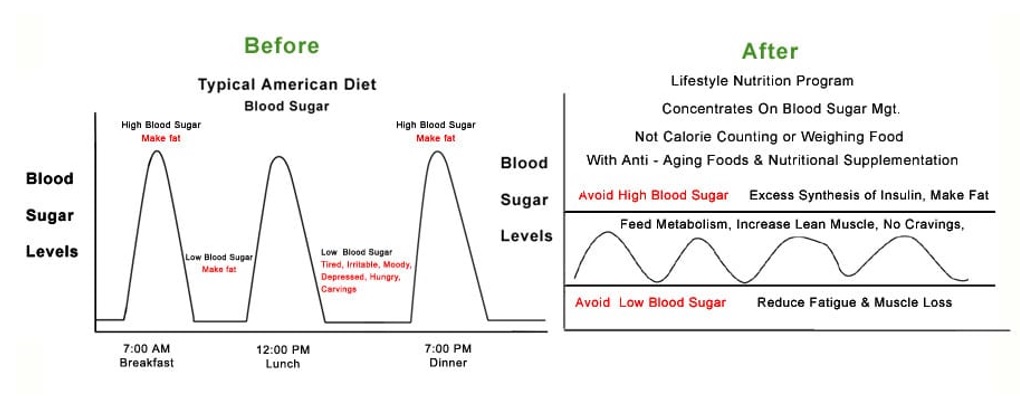
The standard American diet is inflammatory, oxidative and high glycemic, high in trans fats and sugar which promotes many diseases, pre-diseases and problems that your patients searching for guidance to.
1 The prevalence of hyperlipidemias, insulin resistance, weight gain, obesity, pre- diabetes, fatigue, arthritis and pain management are negatively impacted by a poor diet.
2 As practitioners we are faced with contradictory research, nutritional counseling is typically time consuming and it can be difficult to determine the best approach to guide patients. Lastly, many practitioners have implemented various nutritional counseling programs in the past without adequate long term effectiveness and are often disheartened with many nutritional counseling programs.
Interestingly, tougher economic times produce more job, environmental and relationship stress, which often produces more emotional and comfort eating that results in consumers choosing less healthy foods.
3. According to the Center for Science in the Public Interest (CSPI) it costs an average of $1,400 to lose 20 pounds of weight in the US. Most commercialized weight loss programs often use expensive packaged foods, meal replacements, diet products, supplements and are not medically supervised.Nutritional programs incorporating patient’s food preferences and incorporating healthy supermarket food are often less expensive for patients, and are more effective than most commercial weight loss programs (CSPI)
4. Traditional approaches to nutritional counseling have typically used generic pharmaceutical diet sheets and meal plans to instruct patients which can be overwhelming and too restrictive for most people to follow. Furthermore, patients interpret programs using generic diet sheets, meal replacements and packaged foods as “dieting” instead of a true behavioral lifestyle program, which can also contribute to patients relapsing and lead to yoyo dieting syndrome.
A SYSTEMATIC APPROACH FOR A BUSY HEALTH CARE PRACTICE
By using a metabolic analyzer and customizing each patient’s nutritional program based on their specific muscle mass and including anaerobic and aerobic exercise, A MEDICAL ASSISITANT CAN provide a sliding scale of carbohydrates, fats and protein into the meal plan. We use a proprietary metabolic analyzer and simple software to provide custom meal plans which are based on patient’s sex, height, weight, age, lean muscle mass and activity level.

 Metabolic Analyzer
Metabolic Analyzer
Custom Clinical Lifestyle Nutrition Metabolic Meal Plans Improve Compliance – Evidence Based Program
Now medical assistants and designated “wellness coaches” can been trained by Progressive Registered Dietitians / Clinical Nutritionists at Lifestyle Nutrition to utilize software and a metabolic analyzer to quickly develop custom clinical meal plans for metabolic analyzer to quickly develop custom clinical meal plans for based on PATIENTS FOOD PREFERENCES for weight loss, weight gain or weight maintenance &/ or for specific diseases, such as
|
|
A customized program based on lean mass activity level, age and specific exercises will reduce a patient’s hunger level and insulin overload without causing fatigue. Patients now adopt lifestyle changes in a positive way and look forward to their weekly nutritional sessions to incorporate long term behavior modification which is crucial to decrease the likelihood for relapse. Some patients may require shopping lists with foods that can be purchased at a Whole Foods or Trader Joes Supermarket, Kroger ans Safeway and others may be purchasing foods at a Wal-Mart or Costco.
Nutritional Compliance, Metabolic Profiling and Patient Food Preferences – “ A Behavioral Approach”
It is paramount for patient compliance to provide tailored sliding scale meal plans which can change the amount of carbohydrate, fat and protein for each patient’s metabolic profile and activity level. Using a sliding scale meal plan based on the patients metabolic profile, activity level and lean muscle mass assures, we provide the patient with adequate carbohydrate for glucose, muscle glycogen and energy utilization, protein for muscle anabolism and healthy fat for anti-inflammation and satiety. This approach along with exercise has helped decrease the least insulin resistance, hyperlipidemias, fatigue and diabetes, cardiac and cancer risk factors which are prevalent in America. 17.
This approach significantly decreases hunger, appetite, fatigue and your patients will embrace your suggestions and look forward to learning more. Clients are substantially more motivated and receptive to learn how to properly balance their blood sugars rather than just counting calories or dieting. We encourage patients to become more aware of the improvement of their energy levels, stamina, and focus. As a result overall well-being improves rather than the just the number on the scale. By quantifying caloric expenditure based on lean muscle mass and anaerobic and aerobic calorie expenditure, you can be more effective with weight loss, insulin resistance, fatigue and lean muscle mass increases. 15
Most current and traditional metabolic equations used to perform metabolic assessments are often inaccurate because they are based on the body weight of patients instead of lean body muscle mass. 5.

Christopher Fuzy MS, RD, LD Clinical Nutritionistand Assistant Performing Nutritional & Metabolic Assessment
A key component to relapse prevention following rapid weight loss detoxification programs, pharmacologic or HCG rapid weight loss is to provide patients with detailed guidelines as to the reintroduction of real food back into the their lifestyle, so patients do not revert back to old habits and regain the weight they lost. Often, lean muscle mass and metabolic profiles change after weight loss, so retesting patients’ metabolism and lean mass is critical to be able to provide the correct maintenance program.
An effective nutritional program should include behavioral, metabolic, and have the clinical flexibility to support and accommodate various patient backgrounds with different clinical needs. Long –term patient compliance will occur as a result with periodic follow up visits. You will find that introducing an efficacious nutrition counseling program to your patients and community
Good Lifestyle Nutrition Medicine Is Good Business Too
Since patients are not forced into purchasing expensive nutritional products, lifestyle nutrition counseling programs, recommending healthy normal supermarket foods are
1. significantly less costly (more affordable),
2. more profitable,
3. market well in the community and
4. gain respect from peers.
According to the Center for Science in the Public Interest (CSPI) it costs an average of $1,600 to lose 20 pounds of weight in the US, however packaged foods, meal replacements, diet supplement programs are upwards of $4,600 to lose 20 lbs and are not physician supervised. Expected annual costs for the diet pills are $1,743 for Lorcaserin; $1,518 for Orlistat; and $1,336 for Qsymia. Relapse prevention is the primary concern with any medical or nutritional intervention especially when patients have not changed their lifestyle and discontinue purchasing medications, packaged foods, hormones and diet supplements etc..
Nutritional counseling patient PROGRAMS can generate approximately $450 – $3,000 revenue per patient in 3-12 nutritional sessions depending upon the needs of the patient and the socioeconomic status of your geographical location of your practice. These fees are approximately 25-40% the national average for a commercial weight management programs which are not physician supervised! Conservatively an average cash pay patient generates approximately $1,200 revenue or 20 patients monthly can generate $24,000 income monthly without selling any diet products or anything. The cost of having the Lifestyle Nutrition Metabolic Counseling Program in your practice can range between $200 – $600 monthly depending upon the hardware, training, software, marketing and support you desire. 1 patient monthly covers the cost of the program in my practice.
PPO , Medicare Reimbursement for Lifestyle Nutrition Management
PPO’s and Medicare may reimburse for nutrition counseling with specific diagnosis as previously mentioned. Many physicians do not focus with insurance and Medicare reimbursement and obesity patients, however it’s nice to know there is some reimbursement for these patients. Patients can also use their preventative medicine wellness visits for counseling. Also, there are CPT codes for BMI screening, medical nutritional therapy services, V codes for dietary surveillance and behavioral therapy codes for both GROUP OR INDIVIDUAL COUNSELING.
According to the NCD for Treatment of Obesity, at Treatment of Obesity NCD, services performed in connection with the treatment of obesity are covered by Medicare when such services are an integral and necessary part of a course of treatment for diseases and covers therapy for obesity when the guidelines have been met. Obesity is defined as a body mass index (BMI) ≥ 30 kg/m2, for the prevention or early detection of illness or disability.
It’s Not Your Fault – Physicians in the US Were Never “Formally” Trained With Nutrition
Lifestyle Nutrition’s’ webinar and onsite training and support from their Clinical Nutritionists / Dietitians is specific for your practice, patients and nutritional philosophy and patient demographic. Everything can be customized specifically for regional or ethnic foods and background of our many types of patients.
Lifestyle Nutrition Inc® provides the tools to introduce the program to your practice such as posters, custom brochures, surveys, news ads, patient materials, health risk assessments, flyers, articles. They also provide press releases, news ads and even sample TV commercials, web ads and SEO. . Physicians could also provide a corporate wellness screening program or screening to patient’s employers if they wanted to do so. I could also provide a corporate wellness or health fair screening program to my patient’s employers if I wanted to do so. Finally, the training and support from Lifestyle Nutrition® has allowed us to incorporate the program into our practice and create a service that is lucrative, efficacious, and that markets well and is difficult to find in America.
How To Clinically and Financially Evaluate the Lifestyle Nutrition Metabolic Counseling Program For Your Philosophy and Patient Demographic
TO REALISTICALLY EVALUATE THE LIFESTYLE NUTRITION COUNSELING PROGRAM FOR YOUR PATIENTS AND YOUR PRACTICE, COMPLETE FORM SO YOU WILL RECEIVE A ONLINE MEAL PLAN QUESTIONNAIRE AND CAN REQUEST A PRIVATE INTERACTIVE WEBINAR WITH ONE A CLINICAL NUTRITIONISTS TO REVIEW YOU CUSTOM NUTRITION PROGRAM. The webinar will specifically review your personal metabolic and lifestyle nutrition program and then you will be able to effectively evaluate the program for your clinical philosophy and your patient demographic.
Finding An Effective Program Will Be Personally and Financially Rewarding
Finally, one of the most rewarding and lucrative decisions you will make is to implement a credible Lifestyle Nutrition Metabolic Counseling Program in your practice. Providing a Lifestyle Nutrition counseling is rare to find because most programs push products, meds, hormones or rely on counting calories, food groups or carb gram counting etc. Credible behavioral modification programs gain respect from peers, market well and can positively brand your practice apart from other doctors , and nutrition counseling programs in your city. Furthermore, behavior modification program only cost 30-40 % of of most commercialized weight loss programs in the US and are not even medically supervised . Finally patients are more receptive to individualized nutrition counseling and physicians who implement Lifestyle Nutrition Counseling programs report it is a positive uplifting experience for physicians, patients and medical staff.
 Christopher Fuzy, MS, RD, LD is the Founder and President of Lifestyle Nutrition Inc. and LIFESTYLENUTRITIONINC.COM, has a Master’s Degree in Clinical & Sports Nutrition with offices in Ft. Lauderdale and Boca Raton, FL. Over the past 20 years, he has trained over 700 physicians nationwide in the implementation of his Lifestyle Nutrition Counseling Program®. For More Information or to try your own nutritional program, visit LIFESTYLENUTRITIONINC.COM or call 800-699-8106.
Christopher Fuzy, MS, RD, LD is the Founder and President of Lifestyle Nutrition Inc. and LIFESTYLENUTRITIONINC.COM, has a Master’s Degree in Clinical & Sports Nutrition with offices in Ft. Lauderdale and Boca Raton, FL. Over the past 20 years, he has trained over 700 physicians nationwide in the implementation of his Lifestyle Nutrition Counseling Program®. For More Information or to try your own nutritional program, visit LIFESTYLENUTRITIONINC.COM or call 800-699-8106.
www.DoctorsNutritionProgram.com – For Doctors or 800-699-8106
LIFESTYLENUTRITIONINC.COM – Patient Website
Interrelationships among postprandial satiety, glucose and insulin responses and changes in subsequent food intake. Eur J Clin Nutr. 1996 Dec;50(12):788-97. Glycemic index, glycemic load, and chronic disease risk—a meta-analysis of observational studies American Journal of Clinical Nutrition, Vol. 87, No. 3, 627-637, March 2008 |